
Overview
Glenohumeral arthritis is also known as shoulder arthritis. It is a progressive type of arthritis that is normally caused by damage to the cartilage surfaces of the shoulder's glenohumeral (ball and socket) joint.
When this cartilage becomes damaged, it can cause the bones within the joint to rub against each other. This in turn can cause stiffness, discomfort or pain.
How common is it?
Glenohumeral arthritis is a common source of pain and disability among older people and is thought to affect as much as 20% of the older population. It can also affect younger people, though this is less common. Arthritis of the shoulder is less common than in many other joints, such as the hips, knees, and hands.
Why does it happen?
Glenohumeral arthritis can be caused by several factors. These include:
prior shoulder surgery
a history of trauma
over-use of the shoulder (involving intense overhead activities such as weightlifting, bowling in cricket or many racket sports)
inflammatory conditions such as rheumatoid arthritis (a disease where the body's own immune system attacks its joints)
multifactorial causes and probably a genetic predisposition
Symptoms
The most common symptom is pain, which often increases over a period of time. This can go on for as long as several years. You may have pain at rest, although not always, and movement will usually add to your discomfort. Many patients report pain and interrupted sleep at night.
Loss of motion is also common. This may be caused by osteophytes (bony spurs caused by the bone-on-bone friction), or constriction due to inflammation. Fractures, previous surgery, or weakness in the supporting muscles may also have a negative impact on motion.
Other symptoms can include atrophy (wasting away) of the shoulder muscles through lack of use, inflammation of the affected area, tenderness to the touch and a clicking or crunching sound when you move your shoulder.
Investigating the problem
Physical examination
Mr. Cole will talk to you about your shoulder symptoms. He will examine your shoulder and assess your range of movement, whether your shoulder is tender to the touch and whether it makes any sound when moved. It is important to check for the functioning of the rotator cuff muscles
X-ray
An x-ray can provide an excellent "picture" of bones and joints and can provide confirmation of glenohumeral arthritis. Your x-ray may show structural changes to your shoulder such as erosion or irregularity of the joint surface and bone spurs. It is often the only investigation that is necessary.
CT-Scan
CT stands for computerised tomography. It can be used to establish the extent of any bone loss, as well as any anatomical abnormalities that may affect your treatment. A CT scanner uses a series of x-rays taken at slightly different angles of your body, to produce very detailed pictures. It is a non-invasive and painless procedure. It is not done routinely but is necessary if there is significant bony damage.
MRI SCAN
Mr Cole may request a MRI scan to look at the muscles and tendons around the shoulder, particularly the rotator cuff if surgery is contemplated.
Treatment options
There are many treatment options for glenohumeral arthritis, ranging from pain medication and exercises for mild cases, to surgical procedures (shoulder replacement) for severe cases.
Non-surgical treatment
Painkillers
Pain medication and anti-inflammatory medicines will help to ease your symptoms of pain and stiffness. If your symptoms are mild, this may be enough to keep your condition manageable.
Physiotherapy
Physiotherapy will help you maintain motion in your shoulder joint and can prevent the onset of further stiffness. Should you need any other form of treatment, such as injections or surgery; physiotherapy will form an important part of your rehabilitation and recovery.
Injections
Depending on the extent and duration of your arthritis, you may benefit from a steroid or a hyaluronan injection. Steroids (such as cortisone) are good at reducing the inflammation. However, it is unlikely that you will be able to have more than three steroid injections during one year. Depending on your symptoms and presentation, Mr. Cole may recommend a hyaluronan injection. This can help improve joint lubrication and reduce friction during movement.
Exercises
Exercising your shoulder is an important part of your recovery. It can help to minimise stiffness and avoid further possible complications such as muscle atrophy (where your muscles start to waste away because they are not used). An exercise programme will be devised for you by your team of physiotherapists, in conjunction with Mr. Cole. It will last for several weeks and is something you will need to do every day.
Surgical treatment
Should you need surgery, Mr. Cole will advise you on what type of treatment best suits you and your situation. He will choose the most appropriate and least invasive for you.
Arthroscopic treatment
This is a keyhole surgery where a camera is used to help identify and target specific problem areas. It is normally completed as day surgery and is minimally invasive. This may only be possible in very early arthritis and is unlikely to be helpful in more advanced cases.
Shoulder replacement
In more severe cases, Mr. Cole may recommend shoulder replacement. There are different types of shoulder replacement and Mr. Cole will discuss with you the most suitable one for your particular problem. In most cases, a total shoulder replacement (includes replacement of the cup side) is the replacement of choice, but other replacements such as a reverse shoulder replacement, hemiarthoplasty and resurfacing replacements will be discussed.
If Surgery is necessary Mr. Cole will discuss with you the advantage sand disadvantages of each type of shoulder replacement and the best type of shoulder replacement for your individual circumstances.
Exercises
Following your surgery, your team of physiotherapists will work with you to devise an exercise programme. This will be designed with advice from Mr. Cole to help you recover as quickly and efficiently as possible.
Surgery
About shoulder replacement and resurfacing arthroplasty
The most common reasons for replacing the shoulder joint are for arthritis, either osteoarthritis (wear and tear) or rheumatoid arthritis. It may also be necessary following a fracture. Surgery is always the last option and is only used in cases of ongoing pain or where non-surgical treatment has failed to work.
Mr. Cole will discuss the best operation for your shoulder. There are different types of shoulder replacement and surface replacement available. The two types of shoulder replacement most commonly used are total shoulder replacement and hemiarthroplasty. In the hemiarthroplasty procedure a metal prosthesis is implanted into the upper bone of the arm (humerus) which forms the "ball" part of the shoulder's ball and socket joint. In total shoulder replacement, both the ball and socket sides of the joint are replaced. A plastic cup is used for the socket.
A resurfacing replacement involves smoothing down the humeral head (ball part) of the joint and fitting a smooth metal cap over the surface.
Preparing for your operation
If you have shoulder replacement surgery, you will have to stay in hospital for a few days. This is usually less than a week. You may feel more comfortable if you bring your own dressing gown, slippers and toiletries.
During the operation you will be given a general anaesthetic. It is important that you don't eat or drink anything for six hours prior to your admission into hospital, although you may drink water up to two hours
prior to admission.
If you normally wear make-up or nail varnish, please remove it prior to your admission. You will also need to bring all prescribed medicines and supplements, in their original containers, with you to the hospital.
Understanding your operation
After admission, you will be seen by Mr. Cole and by your specialist anaesthetist. They will talk about the operation and the anaesthetic with you and, where possible, discuss your preferences. Nothing will be done
without your permission.
Anaesthetic and pain relief
The operation is carried out under a general anaesthetic. After your admission, you will be given a pre-med. This is usually in tablet or liquid. It will help you relax before your operation.
You will then be taken to the anaesthetic room, where you will be given the anaesthetic. This may either be a gas to breathe or an injection. This will be all you remember about the operation, as you will fall asleep at this point and awake after the operation in the recovery room.
Normally you will be given an interscalene nerve block during the operation. This acts as an excellent pain relief and for a short while after your operation your shoulder and arm may feel numb. When this wears off, your shoulder can feel very sore. You will be given some painkillers to take after the operation. When you begin to feel sensation returning to your shoulder (often a "pins and needles" feeling), you should start taking the pain medication that you have been given. Don't wait for your shoulder to start hurting, as pain is best managed before it gets acute. To keep the pain under control, use your medication regularly to begin with. After a few days, you can begin to lower the amount you take and then cease the medication altogether once any pain has subsided. Although the operation is to relieve pain, it may be several weeks until you begin to feel the benefit. If the pain does not seem to get better, or if you need more pain medication, please contact Mr. Cole. You may have some bruising around your shoulder and upper arm. This will gradually disappear over a period of a few weeks.
A cold compress can also help with pain relief and swelling at the site of your operation. If you use an ice pack it is important you keep the wounds dry. You can repeat this several times a day.
Risks
All operations involve a small element of risk. In shoulder replacement or resurfacing operations, these can include:
Complications relating to the anaesthetic such as sickness, nausea or rarely cardiac, respiratory or neurological issues (less than 1% each, i.e. less than one person out of one hundred).
Infection. These are usually superficial wound problems. Occasionally deep infection may occur many months after the operation (less than 1%).
Unwanted pain or stiffness in or around the shoulder (up to 20%).
Damage to the nerves and blood vessels around the shoulder (less than 1%).
A need to redo the surgery. (After 10 years, 5-10%). Dislocation is very rare. However, as with all joint replacements, the components can loosen. This is not normally a problem until several years after the operation.
Please discuss these issues with Mr. Cole if you would like further information.
Recovery
Follow-up appointments
You will usually be invited to attend an outpatient clinic about two weeks after your operation, where the wound will be examined and your stitches removed. After about three months you will be asked to return so that Mr. Cole can check on your progress. You may discuss any concerns you have during these appointments. Alternatively, should you have a concern, you may telephone Mr. Cole's clinic at any time following your operation.
The wound
You will need to keep the wound dry until it has healed. This normally takes 10 to 14 days. You can wash or shower and use ice packs, but protect the wounds with a waterproof dressing. These will be given to you on your discharge from hospital. Avoid using spray deodorant, talcum powder or perfumes near or on the scar. The dressing and stitches will normally be removed at your first follow-up appointment.
The sling
You will be given a sling to wear immediately following the operation. This is for your comfort. You can take the sling on and off as you wish, although you might find it more comfortable to wear your sling at night. You will not need to wear the sling strapped to your body and you will gradually wear it less over a period of four to six weeks following your operation.
Sleeping

Sleeping may be uncomfortable for a while. It's best to avoid sleeping on the side of your operation. If you choose to lie on the other side, you can rest your arm on pillows placed in front of you. A pillow placed behind your back can help prevent you from rolling onto your operated shoulder during the night. If you are lying on your back to sleep you may find placing a thin pillow or small rolled towel under your upper arm or elbow will enhance your comfort.
Your recovery
Different people recover at different rates. However, you will need to avoid certain movements for the six to eight weeks following your operation. For example, you should avoid moving your arm out to the side and twisting it backwards (in the way you would to put on a shirt or a seatbelt). The trick is to put your operated arm into the shirt first, so that it does not need to reach up behind your back. You should also avoid leaning with your body weight on your arm as you might when getting out of a chair, for example. However, you should not be frightened of moving your arm as much as you can. Gradually these movements will become less painful.
Your recovery can be divided into four phases:
Phase 1
Immediately following your operation, until you are discharged
You will start to move the shoulder with the help of your physiotherapist. However, you will find that most of your post-operative activities will be completed one-handed and you may need some help.When you are discharged from hospital, you will find it more difficult to complete day-to-day activities such as dressing, bathing, hair care, shopping and preparing meals. An occupational therapist will discuss this with you and show you how to be as independent as possible during this time.
Before you are discharged from hospital, the staff will help you plan for how you will manage when you leave. Please discuss any worries with them. We may be able to organise or suggest ways of getting help for when you are home.
Phase 2
After you have been discharged and for up to six weeks after your operation
The pain in your shoulder will gradually begin to reduce and you will become more confident. Wean yourself out of the sling slowly over this time, using it only when you feel necessary. Do not be frightened to try and use your arm at waist level for light tasks. You will be seeing a physiotherapist and doing regular exercises at home to get the joint moving and to start regaining muscle control. If you feel unsure about what you can or cannot do, please discuss this with the physiotherapist. Lifting your arm in front of you may still be difficult at this stage.Phase 3
Between six and 12 weeks following your operation
The pain should be lessening. The exercises are now designed to improve the movement available and get the muscles to work, taking your arm up in the air or away from your body when you are sitting or standing. Overall, you will have an increasing ability to use your arm for daily tasks.Phase 4
From twelve weeks after your operation
You can progress to more vigorous stretches if this is necessary for the activities that you want to do. If the muscles are weak because before the operation the shoulder pain stopped you being able to use them, you should find that you will regain the strength in them with regular exercise. Strength can continue to improve for many months, even up to a year or more. However, unfortunately sometimes the muscles are badly damaged and then you may find it is difficult to regain movement even though you are trying very hard. Even if the muscles will not work properly, the pain in the shoulder joint should still be much less than before your operation and often you can find small "trick" movements that enable you to do what you want to do. Most improvement will be felt in the first six months, but strength and movement can continue to improve for 18 months to two years.
Driving
You may begin driving six to eight weeks after your operation or when you feel comfortable. Check you can manage all the controls and it is advisable to start with short journeys. The seat belt may be uncomfortable to begin with, but your shoulder will not be harmed by it.
In addition, it is a good idea to check your insurance policy. Many insurers will require you to inform them of your operation.
Returning to work
The best time for you to return to work depends on which arm has been operated on, if you need to drive and on the type of work you do. If your job is largely sedentary and uses your non-operated arm, or requires minimal arm movements close to your body, you may be able to return to work between six and eight weeks after your operation. However, if you have a heavy lifting job or one with sustained overhead arm movements you won't be able to work for three to four months. It is best to discuss this with Mr. Cole and with your physiotherapy team.
Returning to sport and leisure activities
Your ability to start these activities will be dependent on pain, range of movement and strength that you have in your shoulder. It is best to start with short sessions involving little effort and then gradually increase the effort or time for the activity. Your physiotherapy team will be able to give advice tailored to you and your situation. As general guidance, however, you can expect to have to wait this long for these sports:
Gentle swimming: after six weeks
Gardening (light tasks such as weeding – do not try to do any digging): six to eight weeks
Bowls: three to four months
Golf, tennis, badminton, squash: four to six months
Physiotherapy
You will be shown exercises by the physiotherapist and you will need to continue with the exercises once you go home. They aim to stop your shoulder getting stiff and to strengthen the muscles around your shoulder. We have outlined these early exercises here. Your physiotherapy team will also devise a longer term programme tailored for you and your situation. Use pain-killers, ice packs or both to reduce any pain before you begin exercise, if necessary. It is better to do short frequent sessions of physiotherapy several times a day, rather than one long session. Aim to exercise for five to ten minutes, four times a day.
It is normal for you to feel aching, discomfort or stretching sensations when doing these exercises. However, intense or lasting pain (such as pain that lasts for more than 30 minutes) is an indication to change the exercise by doing it less forcefully or less often.
Post operative exercises
Phase 1 Exercises
You can begin these exercises immediately after your operation.
1. Pendulum (shown for left shoulder)
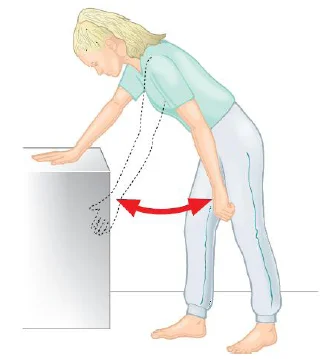
Lean forwards with support
Let your arm hang down
Swing your arm forwards and back
Swing your arm side to side
Swing your arm in circles
Repeat 5–10 times each movement
2. Shoulder shrug (shown for both shoulders)

Sit or stand
Slowly shrug both shoulders up and forwards
Roll them gently down and back
Repeat 10 times
3. Twisting outwards (external rotation) (shown for right shoulder)

Lie on your back, with a folded towel under your operated arm, holding a walking stick, or rolling pin, or umbrella
Keep your elbow into your side throughout
Push with your unaffected arm, so that the hand of your problem side is moving away from the mid-line. Do not over-stretch or let your body twist round to compensate
Repeat 5 times
4. Arm overhead (flexion in lying) (shown for left shoulder)
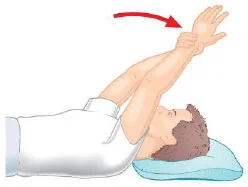
Lie on your back on your bed or the floor
Support the arm of your operated shoulder with your other hand at the wrist and lift it up overhead
Do not let your back arch
Try to get your arm back towards the pillow or floor
You can start with elbows bent and later try it with your arms straight
Repeat 5–10 times
5. Pulley pull (shown for right shoulder)

Sit or stand
Set up a pulley system with the pulley or ring high above you – it is best to have the pulley point behind you
Pull down with your unoperated arm to help life the operated arm up
Repeat 10 times
Phase 2 Exercises
You should do these exercises, as advised by Mr. Cole or your physiotherapy team, from 10-14 days to six weeks following your operation.
1. Arm overhead, with elbows bent (flexion in lying) (shown for right shoulder)

Lie on your back on your bed or the floor, with the elbow of your operated arm bent
Support the arm of your operated shoulder with your other hand at the wrist and lift it up overhead. Once it is vertical, try and keep it there without the support of the other arm
Gradually lower and raise your arm in and arc, until you can lift it from the floor or the bed
Do not let your back arch
Repeat 10 times
2. Arms behind back (shown for right shoulder)

Stand with your arms behind your back
Grasp the wrist of your operated arm
Gently stretch your hand towards the buttock of your un-operated side
Slide your hands up your back
Repeat 5 times
3. Arm across body stretch (shown for left shoulder)
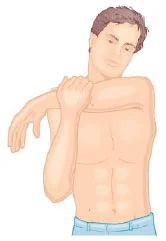
Stand or sit
Take the wrist of your operated arm across your body towards the opposite shoulder
Repeat 5 times
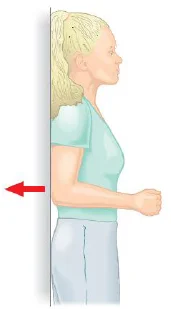
4. Wall hand push (shown for right shoulder)

Stand with your operated arm against a wall
Bend your elbow
Push the back of your hand into the wall, but do not let your arm move
Hold for 10 seconds
Repeat 5 times
Build up to 30 (3x10) repetitions
5. Back-to-wall elbow push (shown for right shoulder)
Stand with your back against the wall
Keep your operated arm close to your side with your elbow bent
Push your elbow back into the wall, but do not let your arm move
Hold for 10 seconds
Repeat 10 times
Build up to 30 repetitions
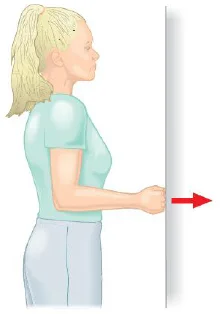
6. Side-to-wall elbow push (shown for right shoulder)
Stand sideways to a wall with your operated arm leaning against the wall
Keep your operated arm close to your side with your elbow bent
Push your elbow against the wall, but do not let your arm move
Hold for 10 seconds
Repeat 10 times
Build up to 30 repetitions
7. Face-to-wall fist push (shown for right shoulder)
Stand facing a wall, about 10cm away from the wall, so that your fist is touching the wall without you needing to move your arm
Keep your operated arm close to your side with your elbow bent to 90 degrees
Push your fist into the wall, but do not let your arm move (use a towel if this is uncomfortable for your hand)
Hold for 10 seconds
Repeat 5 times
Build up to 30 repetitions
8. Wall slide (shown for right shoulder)
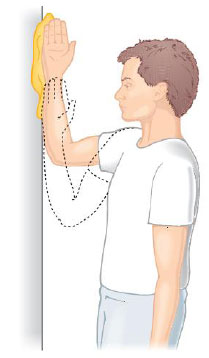
Stand facing a wall with your elbow bent and the side of your hand and arm up to the elbow resting against the wall
Place a paper towel between your hand and the wall (this will make sliding easier)
Slowly slide your hand up the wall
To begin with, you may support your elbow with your other hand
Gradually stretch higher up the wall
Repeat 5 times
Increase to 15-20 repetitions
Progress by standing slightly further away from the wall
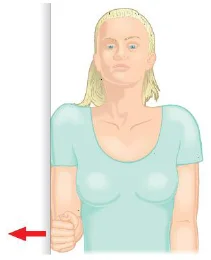
9.

Keep elbow INTO your side.
Start with your hand in front of your stomach and pull hand outwards until it is in front of you.
Control the movement on return and do NOT try and pull out too far.
Repeat 5 times.
Aim to gradually increase to 3x10 repetitions.
10. Hands clasped (shown for right shoulder)

Stand with your elbow bent and your arm close to your side (this can be done against a wall or door frame)
Clasp your hands together and push the palm of your hand into your other hand, taking care to not let it move
Hold for 10 seconds
Repeat 10 times
Build up to 30 repetitions
11. Hands clasped overhead lift (shown for either shoulder)
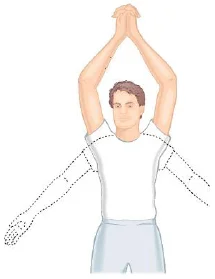
Stand with your hands clasped in front of you
Slowly lift your arms into the air, raising them directly in front of you
Once your arms are overhead, unclasp your arms and lower your arms simultaneously (bend your elbows and lower each one down to your sides)
Repeat 5 times
Progress this exercise by reversing the movement (start by taking your elbows out to the side and lift your arms overhead, clasp your hands and lower to your front)
Progress further by keeping your arms straight
12. Elbow move (shown for either shoulder)
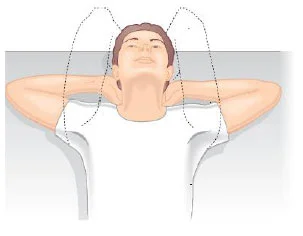
Lie on your back on the bed or the floor
Put your hands behind your neck with your elbows pointing to the ceiling
Slowly relax your elbows so they move apart and lower to the floor or bed
Repeat 3-4 times
Phase 3 Exercises
There is a great variation between what different people can achieve during their rehabilitation, so don't worry if you cannot do these exercises or if your physiotherapist gives you different exercises to try. A special programme will be devised for you by your physiotherapy team in consultation with Mr. Cole. They will concentrate on increasing the strength and mobility of your shoulder and will be designed for your specific needs.
I would like to thank Professor Carr and Jane Moser of the Oxford Shoulder and Elbow Clinic for allowing us to reproduce some of this text and illustrations from their patient information