
Overview
What is frozen shoulder?
Frozen shoulder is a condition where the ball and socket joint of the shoulder appears to "freeze". This causes loss of motion with stiffness in all directions. Typically the shoulder joint is stiff and initially painful. It can often start without an apparent cause.
It occurs when a loose bag, known as a capsule, which surrounds the shoulder joint, becomes inflamed. The bag then appears to tighten or shrink. This tightening combined with the pain restricts movement in the joint and it can be described as "frozen".
There are two main types of frozen shoulder; primary and secondary.
Why does it happen?
In primary frozen shoulder, the exact cause is often not known. It is more common in people with diabetes and with a thyroid gland problem. About 15% of patients link it to a minor injury to the shoulder.
A secondary frozen shoulder can develop if the shoulder area is kept still for some time, for example, after a stroke or heart attack. It can also occur after major injury or surgery to the shoulder.
Some experts think the inflammation starts with a problem in the shoulder itself, others feel it is related to factors away from the shoulder (e.g. stiff neck, or certain diseases). Research is continuing to try and answer some of the questions surrounding the causes of frozen shoulder.
How common is it?
Frozen shoulder is most common in people between the ages of 40 and 70 and tends to occur more often in women than in men. It is estimated to affect at least one person in 50 every year. This amounts to as many as one million people. About one in ten people who develop frozen shoulder will go on to experience similar symptoms in their other shoulder. This normally happens within five to seven years of the first one. However this tends to resolve more quickly than the first.
Symptoms
The symptoms of frozen shoulder often reveal themselves in three distinct phases.
1) Painful phase (which can last from 2 to 9 months)
The pain often starts gradually and builds up. It may be felt on the outside of your upper arm and can extend down to the elbow and even into your forearm.
It can be present at rest and is worse on movements of the arm. Sleep is often affected, as lying on it can be painful or even impossible. During this time movements of the shoulder often begin to be reduced.
During this phase symptoms may be confused or similar to those of subacromial impingement or rotator cuff problems.
2) Stiff phase (which can last from 4 to 12 months)
The ball and socket joint becomes increasingly stiff, particularly on twisting movements such as trying to put your hand behind your back or head. These movements remain tight even when you try to move the shoulder with your other hand or someone tries to move the shoulder for you. It is the ball and socket joint that is stiff. The shoulder blade is still free to move around the chest wall, and you may become more aware of this movement.
3) Recovery phase (which can last from 5 to 26 months)
The pain and stiffness starts to resolve during this phase, and you can begin to use your arm in a more normal way. The total duration of the process is from 12 to 42 months, although the average period is 18-24 months.
The good news is that although the pain and stiffness you experience may be extremely severe, the problem can usually resolve itself. The vast majority of people who have suffered with frozen shoulder find that their symptoms clear up and only a minority report any interference with everyday activities.
For some however the symptoms are very severe. Pain and stiffness lead to considerable problems. Mr Cole will discuss other options for treatment at your consultation.
Investigating the problem
Physical examination
Mr. Cole will talk to you about the onset of your shoulder symptoms. He will examine your shoulder and examine your range of movement. There is normally a very characteristic restriction in movement and typically all movement in all directions is limited
X-ray
An x-ray can provide an excellent "picture" of bones and joints and will show if your shoulder has developed any bone changes. Often this is the only investigation that is needed. If the x ray is normal and the movement is restricted in a typical fashion the likely diagnosis is frozen shoulder.
Occasionally, Mr Cole will suggest an MRI scan, usually to exclude other conditions if there is any other concern.
Treatment options
There are 2 main treatments for frozen shoulder, nonsurgical (conservative) and surgical treatment. Most frequently treatment for frozen shoulder is non-surgical, although a proportion of people do sometimes require or choose an operation.
There is no one agreed treatment option that has been shown to work. Ultimately the shoulder appears to go through the three phases described. The passage of time is often the best treatment. That said, there are treatments that can help you pass through each phase and control difficult areas for you, such as pain. Surgery can increase the range of motion and decrease pain and is generally very successful.
Non-surgical treatment
Painful phase
Pain medication and anti-inflammatory medicines will help to ease your symptoms of pain and stiffness. If your symptoms are mild, this may be enough to keep your condition manageable.
You can also try using heat, such as a hot water bottle, or cold (ice packs). Injections into the joint may also be offered if the pain continues. Physiotherapy at this stage is directed at pain relief (heat, cold and other pain relieving therapies such as electrotherapy). Forcing the joint to move can make it more painful and is best not pursued. You can try using a TENS machine (transcutaneous nerve stimulation) which some people find helpful, or try alternative therapies such as acupuncture.
Stiff phase
Once stiffness is more of a problem than pain, physiotherapy is indicated. You will be shown specific exercises to try and get the ball and socket moving. In addition, your therapist may move the joint for you, trying to regain the normal glides and rolling of the joint. These are known as joint mobilisations. Muscle based movement techniques may also be used.
If movement does not improve with these measures, physiotherapy will be discontinued, although it is appropriate to continue with the suggested
exercises to try and maintain the movement that you do have. Hopefully, as the recovery phase starts you will find that the movement gradually increases. This, again, can be a useful time to have physiotherapy to help maximise the movement.
Surgery
Arthroscopic capsular release (for frozen shoulder)
What is frozen shoulder?
A frozen shoulder is a condition where the ball and socket joint of the shoulder appears to stiffen up and lose movement. This causes loss of motion with stiffness in all directions. Typically the shoulder joint is stiff and initially painful. Pain can be a significant feature of this condition and it can often start without an apparent cause.
It occurs when a loose bag, known as a capsule, which surrounds the shoulder joint, becomes inflamed. The bag then appears to tighten or shrink. This tightening combined with the pain restricts movement in the joint and it can be described as "frozen".
About surgical treatments for frozen shoulder
Most treatment for frozen shoulder is non-surgical, although a very small proportion of people do sometimes require an operation. This is offered to people whose shoulder problem is very slow to resolve or pain is a significant feature. (Remember that frozen shoulder is a self limiting condition which does get better on it's own eventually, however on average it takes 18 months to 2 years to resolve on its own).
If you have significant chronic pain and stiffness Mr. Cole may offer you an Arthroscopic release and manipulation operation. This involves a keyhole procedure which tries to divide and release the loose bag (which is now tight) around your shoulder joint. This is called a capsular release. In addition the joint is stretched in certain directions to try and free the joint up. The operation does not affect any of the muscles and tendons around the shoulder which will continue to work and move the shoulder
About arthroscopic capsular release
This operation is performed by keyhole surgery and aims to release the tight capsule of the joint with a special radio-frequency probe. In addition to releasing the frozen shoulder, Mr. Cole will use the arthroscope (miniature camera) to further examine your shoulder joint for any other lesions or injuries. Although MUA is the traditional operation for frozen shoulder, capsular release is safer and more effective than MUA for people who have developed a persistent frozen shoulder after injury, trauma or fractures, as well as for people with diabetes.
Preparing for your operation
Your arthroscopic capsular release operation will be completed as day surgery. This means that you won't normally have to stay overnight in hospital. However, you may feel more comfortable if you bring your own dressing gown, slippers and toiletries.
You will be having a general anaesthetic. This can make you feel woozy for a short time after the operation, so you will need to arrange for someone to take you home. It is important that you don't eat or drink anything for six hours prior to your admission into hospital, although you may drink water up to two hours prior to admission.
If you normally wear make-up or nail varnish, please remove it prior to your admission. You will also need to bring all prescribed medicines and supplements, in their original containers, with you to the hospital.
Understanding your operation
After admission, you will be seen by Mr. Cole and by your specialist anaesthetist. They will talk about the operation and the anaesthetic with you and, where possible, discuss your preferences. Nothing will be done without your permission on the day.
Anaesthetic and pain relief
The operation is carried out under a general anaesthetic. After your admission, you will be given a pre-med. This is usually in tablet or liquid form. It will help you relax before your operation.
You will then be taken to the anaesthetic room, where you will be given the anaesthetic. This may either be a gas to breathe or an injection. This will be all you remember about the operation, as you will fall asleep at this point and awake after the operation in the recovery room.
Normally you will be given an interscalene nerve block during the operation. This acts as an excellent pain relief and for a short while after your operation your shoulder and arm may feel numb. When this wears off, your shoulder can feel more sore. You will be given some painkillers to take after the operation. When you begin to feel sensation returning to your shoulder (often a "pins and needles" feeling), you should start taking the pain medication that you have been given.
Don't wait for your shoulder to start hurting, as pain is best managed before it gets acute. To keep the pain under control, use your medication regularly to begin with. After a couple of days, you can begin to lower the amount you take and then cease the medication altogether once any pain has subsided. If the pain does not seem to get better, or if you need more pain medication, please contact Mr. Cole.
It is very important in capsular release to start moving the shoulder as soon as possible. Physiotherapy exercises will be started immediately after you operation and should be continued at home. This is a very important factor in getting a successful outcome
A cold compress can also help with pain relief and swelling at the site of your operation. If you use an ice pack it is important you keep the wounds dry.
Risks
All operations involve a small element of risk. In arthroscopic capsular release procedures, these can include:
Complications relating to the anaesthetic such as sickness, nausea or rarely cardiac, respiratory or neurological issues (less than 1% each, i.e. less than one person out of one hundred).
Infection. These are usually superficial wound problems. Very rarely deep infection may occur many months after the operation (less than 1%).
Persistent pain or stiffness in or around the shoulder (10–20% of patients could still have some symptoms after the operation). The stiffness can reoccur
Rarely damage to the nerves and blood vessels around the shoulder (less than 1%).
Please discuss these issues with Mr. Cole if you would like further information.
Recovery
Follow-up appointments
You will usually be invited to attend an outpatient clinic in the following 2 weeks following your operation, where the wounds will be examined and your dressing removed. After about 6-8 weeks you will be asked to return so that Mr. Cole can check on your progress. You may discuss any concerns you have during these appointments. Alternatively, should you have a concern, you may telephone Mr. Cole's clinic at any time following your operation.
The wound
Arthroscopic capsular release is performed by keyhole surgery. This means you will only have two to three small puncture wounds. You will not have any stitches, only small sticking plaster strips. Keep the wounds dry until they are healed, which is normally within five to seven days. You can wash or shower and use ice packs, but protect the wounds with a waterproof dressing; these will be given to you on your discharge from hospital. Avoid using spray deodorant, talcum powder or perfumes near or on the wounds until they are well healed. The dressing will normally be removed at your first follow-up appointment.
The sling
You will be given a sling to wear immediately following the operation. This is for your comfort and can be discarded within a few days. It is very important to take the sling off to start your physiotherapy exercises and prevent the shoulder from becoming stiff again. You might find it more comfortable to wear your sling at night for the first few nights.
Sleeping
Sleeping may be uncomfortable for a while. It's best to avoid sleeping on the side of your operation. If you choose to lie on the other side, you can rest your arm on pillows placed in front of you. A pillow placed behind your back can help prevent you from rolling onto your operated shoulder during the night. If you are lying on your back to sleep you may find placing a thin pillow or small rolled towel under your upper arm or elbow will enhance your comfort.
Different people recover at different rates. However, by about three weeks following your operation you should find that movement below shoulder height becomes more comfortable. You should also be able to move your arm into most positions, including above shoulder height, although this might still be a little painful.
By three months you should feel a lot better. However, it can take from six to nine months to fully recover. You will continue to improve for up to a year following the procedure.
Driving
You may begin driving one week after your operation or when you feel comfortable. Check you can manage all the controls and it is advisable to start with short journeys. You must of course be safe and in control of the car before starting driving.
In addition, it is a good idea to check your insurance policy. Many insurers will require you to inform them of your operation.
Returning to work
The best time for you to return to work depends on how you feel following the operation and on the type of work you do. If your job is largely sedentary with minimal arm movements close to your body, you may be able to return as soon as one week after your operation. However, if you have a heavy lifting job or one with sustained overhead arm movements you may require a longer period of rehabilitation. It is best to discuss this with Mr. Cole and with your physiotherapy team.
Returning to sport and leisure activities
Your ability to start these activities will be dependent on pain, range of movement and strength that you have in your shoulder. It is wise to avoid sustained or powerful overhead movements (such as trimming a hedge, some DIY, racket sports, front crawl) for a few months. In swimming, for example, you should be able to begin breaststroke as soon as you feel able, but you should wait at least three months before attempting front crawl.
It is best to start with short sessions involving little effort and then gradually increase the effort or time for the activity. Your physiotherapy team will be able to give advice tailored to you and your situation.
Physiotherapy
You will be shown exercises by the physiotherapist and you will need to continue with the exercises once you go home. They aim to stop your shoulder getting stiff and to strengthen the muscles around your shoulder. We have outlined these early exercises here. Your physiotherapy team will also devise a longer term programme tailored for you and your situation.
Use pain-killers, ice packs or both to reduce any pain before you begin exercise, if necessary. It is better to do short frequent sessions of physiotherapy several times a day, rather than one long session. Aim to exercise for five to ten minutes, four times a day.
It is normal for you to feel aching, discomfort or stretching sensations when doing these exercises. However, intense or lasting pain (such as pain that lasts for more than 30 minutes) is an indication to change the exercise by doing it less forcefully or less often.
Post operative exercises
Phase 1 Exercises
You can begin these exercises immediately after your operation.
1. Twisting outwards (external rotation) (shown for right shoulder)

Lie on your back, with a folded towel under your operated arm, holding a walking stick, or rolling pin, or umbrella
Keep your elbow into your side throughout
Push with your unaffected arm, so that the hand of your problem side is moving away from the mid-line. Do not over-stretch or let your body twist round
to compensateRepeat 10 times
2. Pendulum (shown for left shoulder)

Do this exercise either standing or lying on your back
Straighten your arm and then bend it at your elbow
Repeat 5 times
3. Arm overhead (flexion in lying) (shown for left shoulder)

Lie on your back on your bed or the floor
Support the arm of your operated shoulder with your other hand at the wrist and lift it up overhead
Do not let your back arch
Try to get your arm back towards the pillow or floor
You can start with elbows bent
Repeat 5–10 times
Progress this exercise by repeating this movement with both elbows bent (with your hands holding the elbows – like a Russian dancer)
Aim to stretch your elbows overhead – remember to avoid arching your back
Repeat 5-10 times
4. Cat-like stretch (shown for either shoulder)

Kneel on all fours
Keeping your hands still, slowly sit backwards towards your heels.
Repeat 5 -10 times
5. Arm overhead (flexion in standing) (shown for right shoulder)

Stand facing a wall with the elbow of your operated shoulder bent and your hand resting against the wall
Slide your hand up the wall, aiming to get a full stretch. (If necessary, use a paper towel between your hand and the wall to make it easier)
Repeat 10 times
Progress by moving away from the wall
6. Pulley pull (shown for right shoulder)

Sit or stand
Set up a pulley system with the pulley or ring high above you – it is best to have the pulley point behind you
Pull down with your un-operated arm to help lift the operated arm up
Repeat 10 times
7. Pushing outwards (shown for right shoulder)

Stand holding a stick or umbrella
Keep your shoulder down
Push with your unaffected arm, so that the hand of your problem side is moving away from the mid-line (you can also do this exercise lying down)
Do not let your body twist round to compensate
Repeat 5–10 times
8. Arms behind back (shown for right shoulder)

Stand with your arms behind your back
Grasp the wrist of your operated arm
Gently stretch your hand towards the buttock of your un-operated side
Slide your hands up your back
Repeat 5 times
9. Arms behind back (with towel) (shown for right shoulder)

Stand holding one end of a small towel with your operated arm behind your back, with your wrist at waist level
Grasp the other end of the towel with your good hand and stretch it above your head
Repeat 5 times
10. Elbow move (shown for either shoulder)
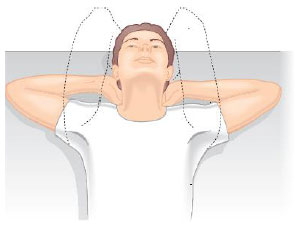
Lie on your back on the bed or the floor
Put your hands behind your neck with your elbows pointing to the ceiling
Slowly relax your elbows so they move apart and lower to the floor or bed
Repeat 5 times
11. Arm across body stretch (shown for left shoulder)

Stand or sit
Take the hand of your operated arm across your body towards the opposite shoulder
Give gentle assistance from your good arm
Repeat 5 times
There is a great variation between what different people can achieve during their rehabilitation, so don't worry if you cannot do these exercises or if your physiotherapist gives you different exercises to try. A special programme will be devised for you by your physiotherapy team in consultation with Mr. Cole.
They will concentrate on increasing the strength and mobility of your shoulder and will be designed for your specific needs. Work hard at your exercises as improvements in strength can increase for up to two years.